
One of the most frightening consequences of stroke is the sudden loss of the ability to speak, understand language, read, or write. A person who was articulate and communicative one moment may be unable to form words, find names for familiar objects, or understand what is being said to them the next. For families and caregivers, witnessing this change can be as distressing as the physical effects of stroke — and often more disorienting, because the person is clearly still present, still thinking and feeling, but suddenly unable to communicate.
Understanding why stroke affects speech and language — what is happening in the brain, which structures are involved, and what forms language loss can take — is the first step toward realistic hope. Because the picture is not as bleak as it can appear in those first hours and days. Language recovery after stroke is possible; it is supported by science, and speech-language pathology is one of the most important tools for achieving it.
At Speech Therapy Centres, our registered speech-language pathologists provide specialised stroke and aphasia rehabilitation for adults across Ontario — in Aurora, Newmarket, Markham, Thornhill, Mississauga, Brampton, Burlington, Ajax, Oshawa, Pickering, Ottawa, and through virtual appointments province-wide.

What Happens to the Brain During a Stroke
A stroke occurs when the blood supply to part of the brain is suddenly interrupted. Without a continuous supply of oxygen and glucose, brain cells begin to die within minutes. The type of stroke determines the mechanism:
- Ischaemic stroke (approximately 87% of strokes): A blood clot blocks an artery supplying blood to the brain. The territory of brain tissue supplied by that artery begins to lose function as cells are deprived of oxygen.
- Haemorrhagic stroke: A blood vessel ruptures, causing bleeding into or around the brain. The bleeding itself damages surrounding tissue, and the accumulated blood exerts pressure on adjacent brain structures.
- Transient ischaemic attack (TIA): A brief, temporary interruption of blood flow that resolves within minutes to hours. TIA produces transient symptoms — including temporary speech difficulty — but by definition does not cause permanent brain damage. It is, however, a serious warning sign of impending stroke.
When the affected brain territory includes areas responsible for language processing, speech production, or the motor control of speech, language and communication impairments result. The specific impairments depend on exactly where in the brain the damage has occurred and how extensive that damage is.
Key statistic: Approximately one third of stroke survivors experience some form of communication difficulty — making aphasia one of the most common and impactful consequences of stroke. In Canada, over 50,000 strokes occur each year, with communication impairment affecting a substantial proportion of survivors.
Where Language Lives in the Brain
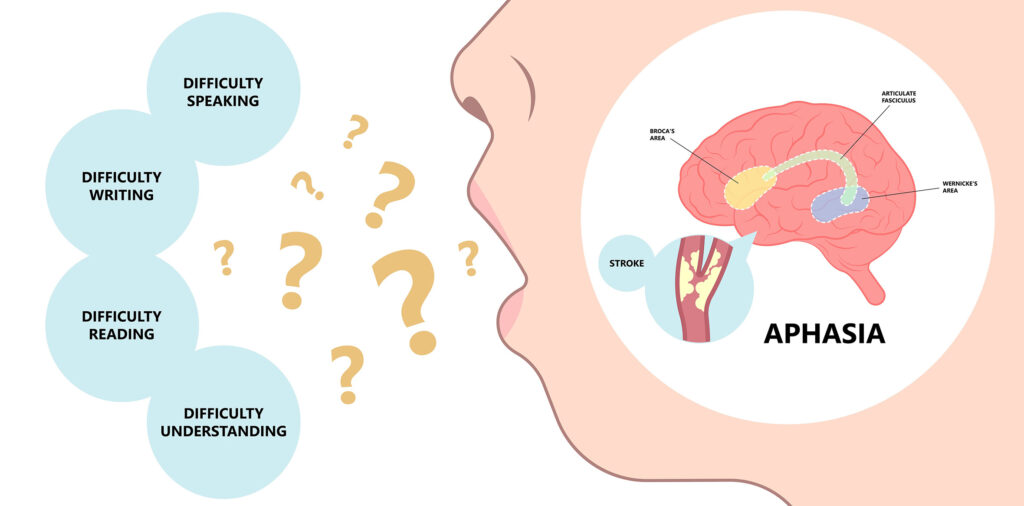
brain regions speech language stroke Broca Wernicke — aphasia anatomy
Language is not stored in a single location. It is processed by a distributed network of interconnected brain regions — predominantly in the left cerebral hemisphere for the vast majority of right-handed people and most left-handed people. The key structures in this language network include:
Broca’s Area
Located in the left inferior frontal gyrus (Brodmann areas 44 and 45), Broca’s area is primarily responsible for speech production and language formulation — the process of converting intended meaning into spoken or written language. It is named for the French neurologist Paul Broca, who in 1861 identified this region’s role in speech production through observations of patients who had lost the ability to speak fluently following left frontal lobe damage.
Damage to Broca’s area results in Broca’s aphasia — characterized by effortful, non-fluent speech with relatively preserved comprehension. The person knows what they want to say but struggles to produce it.
Wernicke’s Area
Located in the left posterior superior temporal gyrus (Brodmann area 22), Wernicke’s area is primarily responsible for language comprehension — the process of decoding and understanding spoken and written language. Named for Carl Wernicke, who described the area’s role in 1874.
Damage to Wernicke’s area results in Wernicke’s aphasia — characterised by fluent speech that is largely meaningless or filled with errors, combined with severely impaired comprehension. The person may speak at a normal rate and melody, but the output is largely incomprehensible and they have limited awareness that this is the case.
The Arcuate Fasciculus
A bundle of white matter fibres connecting Broca’s and Wernicke’s areas — the information highway of the language network. Damage to this pathway results in conduction aphasia, in which comprehension and spontaneous speech are relatively preserved but the ability to repeat words and sentences is severely impaired.
The Angular Gyrus and Supramarginal Gyrus
Regions in the left parietal lobe involved in reading, writing, and the integration of language with other cognitive processes. Damage here contributes to alexia (reading impairment) and agraphia (writing impairment).
The Motor Cortex and Supplementary Motor Area
The primary motor cortex controls the precise motor movements of the lips, tongue, soft palate, and larynx required for speech articulation. The supplementary motor area is involved in the initiation of voluntary movement, including speech. Damage in these areas does not typically affect language processing but results in motor speech disorders — dysarthria and apraxia of speech — that affect the physical production of speech sounds.
Right Hemisphere Language Contributions
While the left hemisphere dominates language processing for most people, the right hemisphere contributes to important aspects of communication: interpreting tone of voice and prosody, understanding implied meaning and humour, processing narrative and discourse, and interpreting facial expressions and body language. Right hemisphere stroke can produce a distinct communication profile sometimes called right hemisphere communication disorder — subtle but real communication changes that can affect social interaction and daily function.
The American Journal of Speech-Language Pathology documents the neuroscience of language recovery after stroke, noting that rehabilitation-driven neuroplasticity — the brain’s ability to reorganize function in response to therapeutic input — is the primary mechanism by which language improves with speech-language pathology intervention.
Types of Aphasia After Stroke
Aphasia is the general term for language impairment following brain damage, most commonly stroke. It is important to understand that aphasia is a language disorder, not an intellectual disorder. Intelligence, personality, and the person’s inner life remain intact; it is the machinery of language — speaking, understanding, reading, writing — that is damaged.
The type of aphasia a person develops depends on the location and size of the stroke. The main clinical aphasia types are:
Broca’s Aphasia (Non-Fluent, Expressive)
The most recognisable form of aphasia for many families. The person has significant difficulty producing speech — output is effortful, slow, and often reduced to single words, short phrases, or telegraphic speech (content words without grammatical structure: ‘wife… hospital… go’). Comprehension is relatively preserved for conversation, though complex syntax may be difficult to process.
People with Broca’s aphasia are typically aware of their language difficulties, which can produce significant frustration and emotional distress. They know what they want to say — the message is intact — but the path from intention to spoken output is disrupted.
Wernicke’s Aphasia (Fluent, Receptive)
Speech output is fluent — normal or even increased rate, normal melody and prosody — but the content is disordered. Output may contain paraphasias (word substitution errors: ‘chair’ for ‘table’), neologisms (made-up words), or jargon (strings of sounds that follow the rhythm of language but carry no meaning). Comprehension is severely impaired — the person cannot reliably understand what is said to them.
People with Wernicke’s aphasia often have limited awareness of their language errors, which can make communication particularly challenging for families, who may find it difficult to understand why the person does not recognize that communication is breaking down.
Global Aphasia
The most severe form, typically resulting from large left hemisphere strokes affecting both frontal and temporal language regions. Both expression and comprehension are severely impaired. The person may produce only a few recurring utterances or sounds. Non-verbal communication — facial expression, gesture, tone of voice — often remains relatively preserved and becomes the primary means of connection.
Despite the severity of global aphasia, meaningful communication and quality of life can be supported through intensive SLP intervention, AAC (augmentative and alternative communication) strategies, and family communication training.
Conduction Aphasia
Comprehension is relatively preserved; spontaneous speech is generally fluent with some paraphasic errors. The characteristic impairment is in repetition — the person cannot accurately repeat words or sentences even when they can understand and produce similar language spontaneously. Results from damage to the arcuate fasciculus connecting Broca’s and Wernicke’s areas.
Anomic Aphasia
The mildest and most common residual aphasia type — often the end-point of recovery from more severe initial aphasia. Speech is fluent and grammatically intact, comprehension is good, but word-finding is significantly impaired. The person knows the word they want, can sometimes describe it or work around it, but cannot consistently retrieve it on demand. This is the type of aphasia that often persists as a subtle but frustrating long-term communication change.
Primary Progressive Aphasia (PPA)
Unlike the aphasias described above, PPA is not caused by stroke. It is a neurodegenerative condition in which language declines gradually over months and years due to progressive atrophy of the language network. It is included here for completeness — speech-language pathology plays a supportive and compensatory role in PPA, though the treatment goals and trajectory differ significantly from stroke-related aphasia.
Important distinction: Aphasia is a language disorder — affecting the ability to process and produce language. It is different from dysarthria (a motor speech disorder causing slurred or imprecise speech) and apraxia of speech (a motor programming disorder affecting the coordination of speech movements). These conditions often co-occur with aphasia after stroke, but require different assessment and treatment approaches.
Motor Speech Disorders After Stroke: Dysarthria and Apraxia
Not all speech changes after a stroke are language disorders. Two motor speech disorders frequently occur following stroke and are distinct from aphasia:
Dysarthria
Dysarthria results from weakness, paralysis, or incoordination of the muscles used for speech — the lips, tongue, soft palate, vocal folds, and respiratory muscles. The person knows what they want to say and can formulate the message correctly, but the physical execution of speech is impaired. Speech may sound slurred, imprecise, breathy, strained, or hypernasal depending on which muscle groups are affected.
Dysarthria is treated by SLPs with exercises targeting respiratory support, articulatory precision, vocal quality, and speech rate modification. Communication supports such as voice amplification or alphabet supplementation may be recommended for more severe presentations.
Apraxia of Speech
Apraxia of speech is a motor programming disorder — the brain’s ability to plan and sequence the precise movements needed for speech is disrupted, even though the muscles themselves are not paralyzed or weak. The person may struggle inconsistently to produce sounds and words, make groping movements with the lips and tongue as they search for the right motor pattern, and produce the same word differently on different attempts.
Apraxia of speech frequently co-occurs with Broca’s aphasia, making assessment and treatment more complex. Evidence-based treatments for apraxia — including DWORKIN-CULATTA oral motor therapy, PROMPT, and intensive motor learning approaches — are provided by specialist SLPs.
Speech Therapy Centres’ registered SLPs are experienced in assessing and treating the full range of communication disorders following stroke, including aphasia, dysarthria, and apraxia of speech. Learn more about our stroke therapy and aphasia services.
Other Communication Effects of Stroke
Beyond aphasia and motor speech disorders, stroke can affect communication in several additional ways:
Dysphagia (Swallowing Difficulties)
Swallowing is controlled by a complex network of brain regions, and stroke — particularly brainstem stroke — frequently disrupts the swallowing mechanism. Dysphagia increases the risk of aspiration (food or liquid entering the airway), aspiration pneumonia, dehydration, and malnutrition. SLPs are the primary clinicians responsible for swallowing assessment and management following stroke.
Cognitive-Communication Disorders
Stroke can affect the cognitive foundations of communication — attention, memory, processing speed, executive function, and social cognition — in ways that produce communication difficulties even without focal aphasia. A person may have difficulty following conversation in a group, keeping track of a narrative, organizing their thoughts for expression, or interpreting indirect language and humour. These cognitive-communication changes are particularly common following right hemisphere stroke and frontal lobe damage.
Voice Changes
Some stroke survivors experience changes in vocal quality — breathiness, reduced loudness, hoarseness, or difficulty projecting the voice — related to vocal fold paresis or changes in respiratory support for speech. SLPs assess and treat these voice changes as part of comprehensive stroke communication rehabilitation.
For patients experiencing voice changes after stroke, our voice therapy services provide targeted assessment and treatment for vocal quality, breath support, and communication projection.
Neuroplasticity: Why Language Recovery Is Possible

The brain is not a fixed, static organ. It has a remarkable capacity for reorganisation in response to experience, learning, and rehabilitation — a property called neuroplasticity. Following a stroke, neuroplasticity is the biological foundation of language recovery.
Recovery through neuroplasticity occurs through several mechanisms:
- Perilesional reorganisation: Brain tissue immediately surrounding the damaged area may take over some of the functions previously performed by the destroyed tissue, particularly in the first weeks to months after stroke.
- Right hemisphere recruitment: The right hemisphere contains homologous language areas that are normally suppressed by the dominant left hemisphere. Following left hemisphere stroke, these right hemisphere regions may be recruited to support language processing, particularly for comprehension and single-word retrieval.
- Strengthening of alternative pathways: The language network contains multiple parallel processing pathways. When the primary pathway is damaged, intensive language stimulation through speech therapy can strengthen alternative routes that become more efficient with practice.
- Synaptogenesis and dendritic growth: Intensive, repeated language practice stimulates the formation of new synaptic connections and dendritic growth in surviving neurons adjacent to and remote from the lesion site.
Critically, neuroplasticity is use-dependent: it is driven by the intensity, frequency, and specificity of language practice. This is why speech-language pathology is essential to language recovery after stroke — passive recovery (simply waiting for the brain to heal) produces significantly less improvement than active, targeted rehabilitation. The brain reorganizes around what it practises.
Speech-Language & Audiology Canada (SAC-OAC) recommends intensive speech-language pathology intervention beginning as early as medically feasible after stroke, noting that both early intervention and continued long-term rehabilitation produce clinically meaningful improvements in communication function through neuroplastic mechanisms.
How Speech-Language Pathology Supports Recovery After Stroke
Speech-language pathology is not a single treatment — it is a specialised clinical process that begins with comprehensive assessment and evolves through multiple stages of recovery. At Speech Therapy Centres, our SLPs provide:
Comprehensive Communication Assessment
Before any treatment begins, a thorough assessment establishes the nature and severity of the communication impairment. Standardised aphasia batteries, motor speech assessments, swallowing evaluations, and cognitive-communication screenings create a detailed profile of what is impaired, what is preserved, and what communication strengths can be built upon.
Aphasia Therapy
The goal of aphasia therapy is to maximize functional communication through a combination of restitution (retraining damaged language processes), compensation (developing strategies that work around impaired processes), and adaptation (modifying communication environments and partner behaviours). Evidence-based approaches used by our SLPs include:
- Constraint-induced language therapy (CILT): Intensive practice that constrains use of compensatory strategies, forcing the patient to practise verbal communication at the edge of their current ability — a high-intensity, neuroplasticity-driven approach.
- Treatment of underlying forms (TUF): Targets complex syntactic structures in a way that generalises to broader grammatical improvement — particularly useful for agrammatic Broca’s aphasia.
- Script training: Intensive rehearsal of personally meaningful conversational scripts builds fluency and automaticity for communication in specific high-priority situations.
- Semantic feature analysis: A structured word-finding therapy that strengthens the semantic network around target words, improving retrieval through associated features.
- Conversational coaching: Training in supported conversation techniques — for both the person with aphasia and their communication partners — to maximise the efficiency of real-world communication exchanges.
Augmentative and Alternative Communication (AAC)
For people with severe aphasia or those in the early stages of recovery, AAC provides access to communication when verbal expression is not yet possible. This ranges from low-tech options (communication books, alphabet boards, gesture systems) to high-tech speech-generating devices and tablet-based applications. Our SLPs assess AAC needs and implement systems that support communication right now, while language rehabilitation continues.
Dysphagia Management
Where swallowing is affected by stroke, our SLPs provide instrumental assessment (videofluoroscopic swallowing study, flexible endoscopic evaluation), texture and consistency recommendations to maintain safe oral intake, and swallowing rehabilitation exercises to restore function over time.
Family and Caregiver Education
The communication environment surrounding a person with aphasia is as important as the therapy itself. Our SLPs work with family members and caregivers to develop supported conversation skills — how to slow down, give time, reduce background noise, use drawing and gesture, confirm understanding, and avoid talking on behalf of the person. Families who are trained to communicate effectively with their loved one become active participants in daily communication practice.
Read more about our comprehensive approach to stroke therapy and aphasia rehabilitation at Speech Therapy Centres, including information about our assessment process and what families can expect.
Language Recovery After Stroke: What to Expect
Recovery from aphasia is not linear — and it is not time-limited in the way that was once believed. The old clinical teaching was that significant recovery occurred only in the first 3 to 6 months after stroke. Research over the past two decades has substantially revised this view. While the period immediately following stroke — sometimes called the acute and subacute phase — does represent a window of heightened neuroplasticity, meaningful language improvement has been documented years and even decades after stroke with appropriate therapy.
Acute Phase (0 to 4 weeks)
In the days and weeks immediately after stroke, spontaneous recovery occurs as swelling resolves, circulation is partially restored, and surviving neurons in the perilesional zone stabilize. SLP assessment in the acute phase establishes a baseline and initiates early supported communication and swallowing management. Intensive language therapy during this phase takes advantage of the heightened neuroplasticity of the early recovery period.
Subacute Phase (1 to 6 months)
This is typically the period of most rapid change. Intensive outpatient speech-language pathology during the subacute phase — ideally 3 to 5 sessions per week — produces the greatest rate of improvement. Goals focus on retraining core language functions, building compensatory strategies, and developing communication supports for daily life.
Chronic Phase (Beyond 6 months)
Contrary to outdated clinical assumptions, language improvement continues well into the chronic phase for people who receive appropriate therapy. Goals shift progressively toward functional communication in real-world contexts, participation in valued activities, community reintegration, and maintenance of communication gains. Periodic intensive therapy blocks — concentrated periods of high-frequency therapy — can produce further gains even years post-stroke.
For families: There is no expiry date on speech therapy after stroke. If your loved one received speech therapy in the acute hospital setting or early rehabilitation but feels that further progress could be made, an outpatient SLP assessment is worth pursuing regardless of how much time has passed since the stroke.
Research reviewed by the American Journal of Speech-Language Pathology demonstrates that intensive aphasia therapy produces statistically and clinically significant improvements in language function in the chronic phase — with greater intensity consistently associated with greater outcomes at all stages of recovery.
Communication Tips for Families of Stroke Survivors with Aphasia
The way family members and caregivers communicate with a person with aphasia directly affects how much communication occurs and how much of the person’s preserved language can be accessed. These evidence-based strategies make a meaningful difference:
- Give time: The most important accommodation. Aphasia slows the pace of language processing and production significantly. Silence does not mean the person has nothing to say — it means they need more time to access and produce it. Resist the urge to fill the silence or complete sentences.
- One idea at a time: Reduce the length and complexity of what you say. Use simple, clear sentences with one idea each. Pause between ideas. Confirm understanding before moving on.
- Use all communication channels: Gesture, pointing, drawing, writing key words, and facial expression all supplement verbal communication effectively. Encourage the person with aphasia to use these channels too.
- Ask yes/no questions when needed: When open-ended communication is difficult, asking questions that can be answered with yes or no, a nod, or a gesture maintains participation and connection.
- Never assume incomprehension: Many people with aphasia, including those with severe expressive impairment, understand far more than they can express. Speak to them as the intelligent adult they are — about current events, family news, opinions, and preferences. Aphasia does not affect intelligence.
- Reduce background noise: Television, radio, and competing conversations make language processing harder for everyone — but particularly for people with aphasia. Reduce auditory competition during important conversations.
- Avoid speaking for them: It can be faster and less frustrating in the moment to complete the person’s sentence or answer for them — but this removes the communication practice that drives recovery and reduces the person’s communicative agency.
Speech Therapy Centres: Stroke and Communication Services Across Ontario
Speech Therapy Centres provides a comprehensive range of communication services for adults following stroke and acquired brain injury. In addition to aphasia therapy and stroke rehabilitation, our SLPs provide assessment and treatment for dysphagia, dysarthria, apraxia of speech, cognitive-communication disorders, and voice therapy for vocal changes following stroke. For families with children who have additional communication needs, our team also provides speech-language pathology for autism spectrum disorder (ASD) — making Speech Therapy Centres a comprehensive resource for the full spectrum of communication needs across the lifespan.
All services are available in-person at our clinic locations across Ontario and through virtual appointments province-wide. Virtual speech-language pathology for aphasia is evidence-supported and has the added advantage of allowing therapy to take place in the patient’s home environment, where generalisation of communication gains is most direct.
Serving Stroke Survivors and Families Across Ontario. At Speech Therapy Centres, we work with stroke survivors and their families from Aurora, Newmarket, Markham, Thornhill, Mississauga, Brampton, Burlington, Ajax, Oshawa, Pickering, Ottawa, and communities across the GTA and Ontario. Our registered speech-language pathologists specialise in aphasia rehabilitation, dysphagia, and cognitive-communication disorders following stroke — providing evidence-based care that is tailored to each person’s unique recovery goals. Book a consultation today to speak with an SLP about your or your loved one’s recovery.
Frequently Asked Questions: Stroke, Aphasia, and Speech Therapy
Can a person fully recover from aphasia after stroke?
Full recovery is possible for some people, particularly those with mild initial aphasia, smaller lesions, and who receive early, intensive rehabilitation. For many people, recovery is substantial but not complete — meaning they achieve functional communication and return to valued activities even if some residual word-finding difficulty persists. The degree of recovery depends on the location and size of the brain injury, the person’s age and health, and the intensity and consistency of speech-language pathology intervention.
How soon after a stroke should speech therapy begin?
As soon as medically feasible — typically within the first days of hospitalization when the patient is medically stable. Early initiation of speech-language pathology assessment and intervention takes advantage of the heightened neuroplasticity of the acute and subacute recovery period. In hospital settings, SLPs assess communication and swallowing from the earliest days post-stroke. Outpatient rehabilitation should begin as soon as the person is discharged.
Is it too late to start speech therapy years after a stroke?
No. While the most rapid period of spontaneous recovery occurs in the first months after stroke, research clearly shows that speech therapy produces meaningful improvements in the chronic phase — years after the stroke. Motivation, appropriate therapy intensity, and a skilled SLP are the key factors for late recovery, not time elapsed since stroke.
What is the difference between aphasia and dementia?
Aphasia is a language disorder caused by focal brain damage — most commonly stroke. Intelligence, memory, and overall cognition are largely preserved. Dementia is a progressive, generalized cognitive decline that eventually affects language alongside memory, reasoning, and daily function. Primary progressive aphasia (PPA) is a form of dementia that begins with isolated language decline, but this is distinct from stroke-related aphasia in its cause, progression, and management.
Can aphasia affect reading and writing as well as speaking?
Yes. Aphasia is a disorder of language — not just speech. Reading (alexia) and writing (agraphia) are frequently affected alongside speaking and comprehension, because they depend on the same underlying language network. The degree to which reading and writing are affected varies by aphasia type and severity. SLPs specifically assess and treat reading and writing as part of aphasia rehabilitation.
What is AAC and would it help someone with severe aphasia?
Augmentative and alternative communication (AAC) refers to all forms of communication other than natural speech — including communication books, alphabet boards, gesture systems, and high-tech speech-generating devices. AAC is highly beneficial for people with severe aphasia, providing a means of communication while language rehabilitation continues. Research consistently shows that AAC does not reduce motivation to regain speech — it supports communication and quality of life throughout the recovery process.
Does Speech Therapy Centres offer virtual aphasia therapy?
Yes. Virtual speech-language pathology is available province-wide through Speech Therapy Centres and is supported by research as effective for aphasia rehabilitation. Virtual therapy has the advantage of taking place in the patient’s home — the environment where communication needs to function — which can support generalisation of gains. It also removes transportation barriers for people with post-stroke mobility limitations.
How do I access stroke and aphasia speech therapy at Speech Therapy Centres?
Contact Speech Therapy Centres directly to book an initial assessment. A physician referral is not required to begin speech-language pathology services in Ontario. Our clinic locations across the GTA and Ontario, as well as our virtual service, make access possible for most families across the province.
Book a Stroke and Aphasia Speech Therapy Assessment — Across Ontario
If you or a family member has experienced a stroke and is struggling with speech, language, or communication, speech-language pathology can make a meaningful difference — at any stage of recovery, not just immediately after the event.
Speech Therapy Centres offers stroke therapy and aphasia rehabilitation in Aurora, Newmarket, Markham, Thornhill, Mississauga, Brampton, Burlington, Ajax, Oshawa, Pickering, Ottawa, and virtually province-wide.
📍 Locations: Aurora | Newmarket | Markham | Thornhill | GTA | Mississauga | Brampton | Burlington | Ajax | Oshawa | Pickering | Ottawa
📅 Book a consultation today at speechtherapycentres.com/stroke-therapy-and-aphasia/
Disclaimer: This blog is for informational and educational purposes only and does not constitute medical advice. Please consult a registered speech-language pathologist or medical professional for a personalised assessment and care plan.